A Comprehensive Guide to the Infrasternal Angle & Compensation Layers
Dec 29, 2021
The Infrasternal Angle is a concept that is gaining popularity on the internet but is a bit of a complicated subject. If appreciated and utilized properly, the Infrasternal Angle can give us significant insight into what a given person is capable of as well as how they compensate in their movement and posture.
In this article, I will discuss:
- What the Infrasternal Angle represents
- Differentiating between Wide and Narrow infrasternal angle presentations
- Common compensations of both infrasternal angle archetypes
- Exercises to help improve the limitations of common infrasternal angle compensation patterns
If you'd rather watch than read, see below:
What is the Infrasternal Angle (ISA)?
The Infrasternal Angle (ISA) is a representation of an individual’s respiratory strategy. There are only two: inhalation and exhalation, also commonly referred to as expansion and compression.
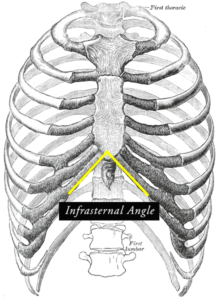
The ISA reflects the strategy the body is using to most easily direct air in and out via the path of least resistance. The infrasternal ribs are the lower ribs that act as a “bucket handle”, and are the most pliable (“changeable”) in the entire axial skeleton.
They are easily reformed because they don’t attach as firmly on the sternum as the upper ribs that act as a “pump handle” upon inhalation.
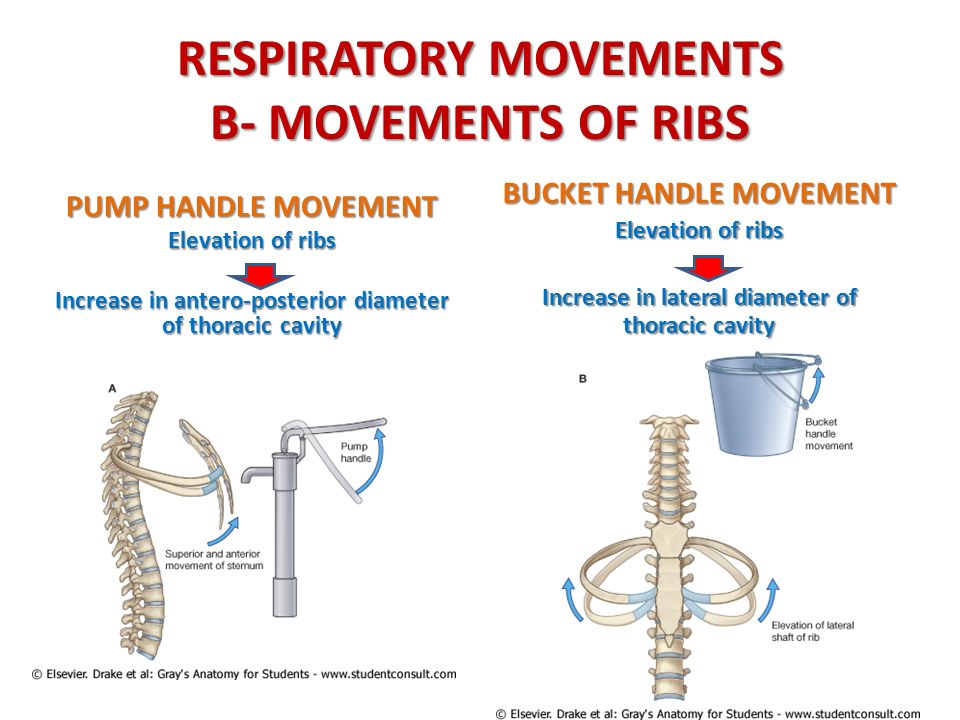
Under normal inhalation mechanics, when we inhale, the diaphragm contracts and descends, which creates a pressure gradient change in the ribcage and allows the ribs to expand (ribcage external rotation) in all directions: Front, back, up, down, outward, and inward.
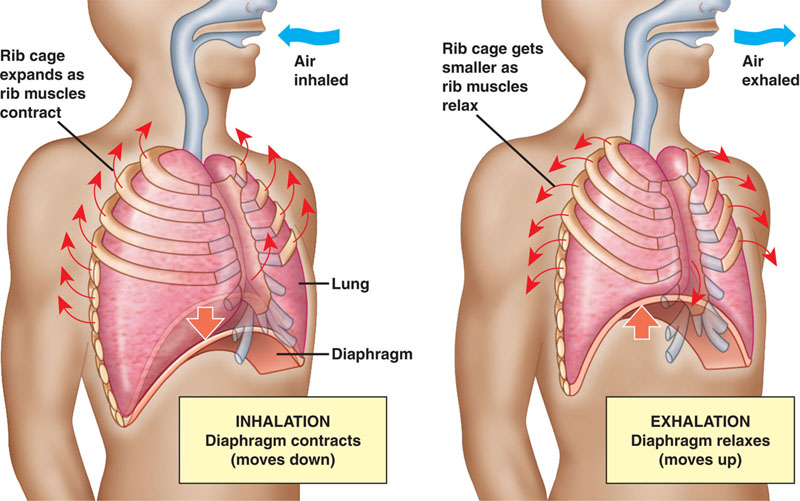
The belly should also simultaneously rise alongside that, but the important thing is that the ribcage needs to also expand in all directions for optimal mechanics of the diaphragm, as well as the pelvic floor.
Infrasternal Angle Archetypes
Everyone knows not every human has the same body type. We inherently recognize that some people have more “narrow” frames and others have more “wide” frames. In the ISA archetype model crated by Bill Hartman, there are two primary types of infrasternal angle presentations: Wide and Narrow.
Wide Infrasternal Angle Archetype
A wide infrasternal angle (usually over ~110 degrees), is reflective on an individual who has an exhaled, or "compressed" axial skeleton. Their ribcage cannot easily expand with air because their axial skeleton as a whole is biased towards exhalation, particularly their back (posterior) ribcage.
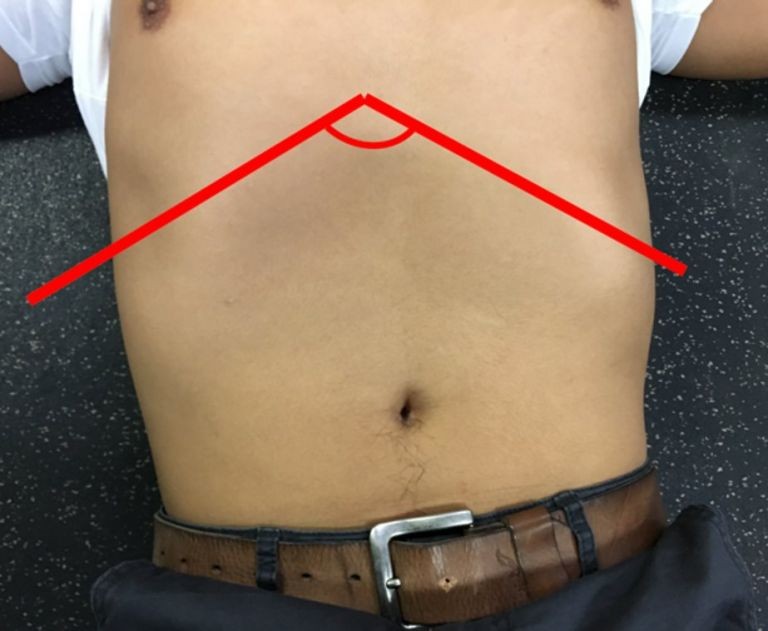
Image credit: Zac Cupples
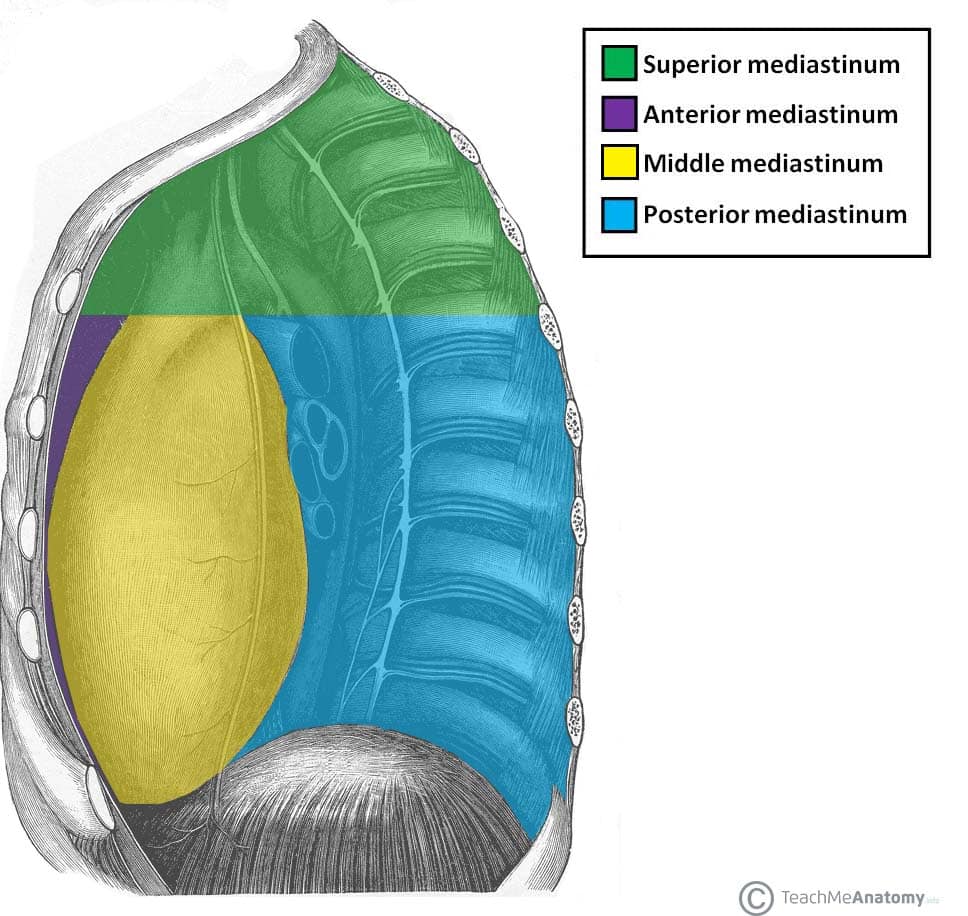
In “normal” breathing mechanics we have cavities in our trunk that have space for the lungs and air to expand into. The posterior ribcage actually has a much, much larger space for this to occur:
Because they struggle to inhale into their ribcage, they’ve created a strategy to expand, or widen out, their ISA in order to take in air. This person is likely a “belly breather” who is able to expand their lower “bucket handle” ribs more than any other portion of their ribcage.
That means their ribs are in a position of internal rotation, which is also their overall joint bias in their whole skeleton.
For many, many years, the fitness and biomechanical industry has associated internal rotation with the joint actions of:
- Extension
- Adduction
- Pronation
- Dorsiflexion
Therefore, we would expect to see these Wide ISAs have more access (initially) to these joint actions.
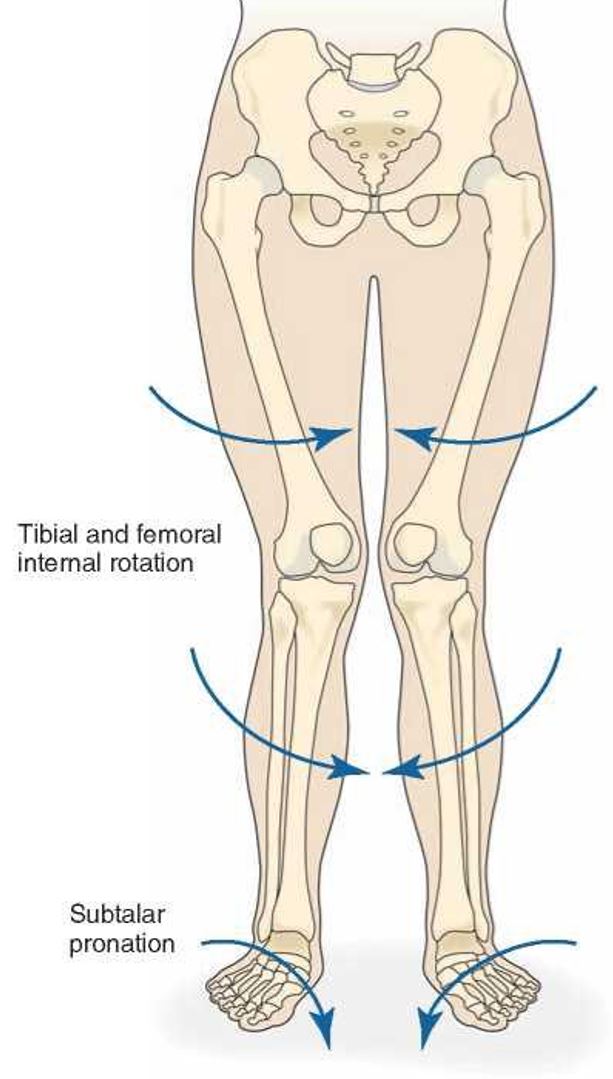
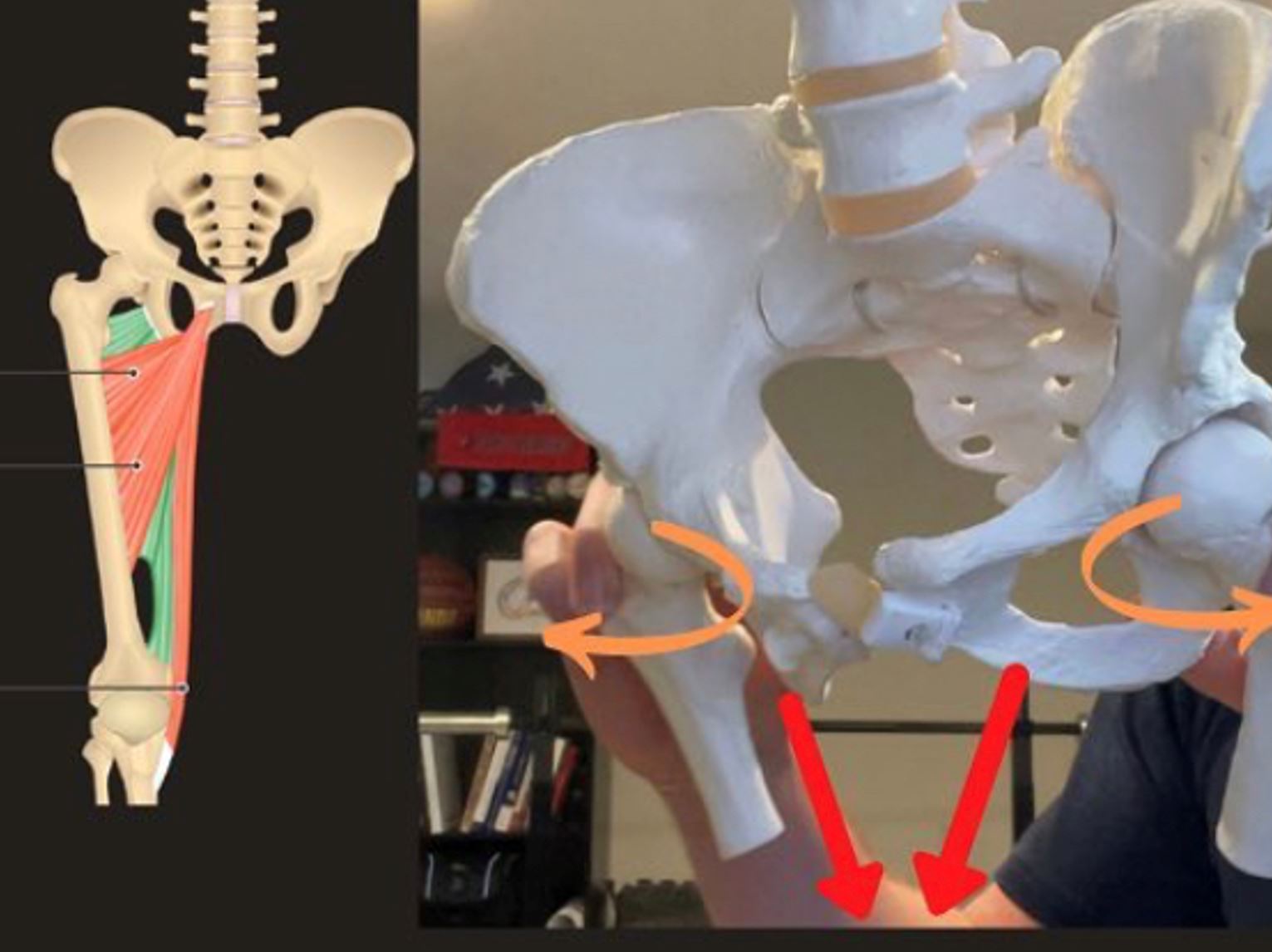
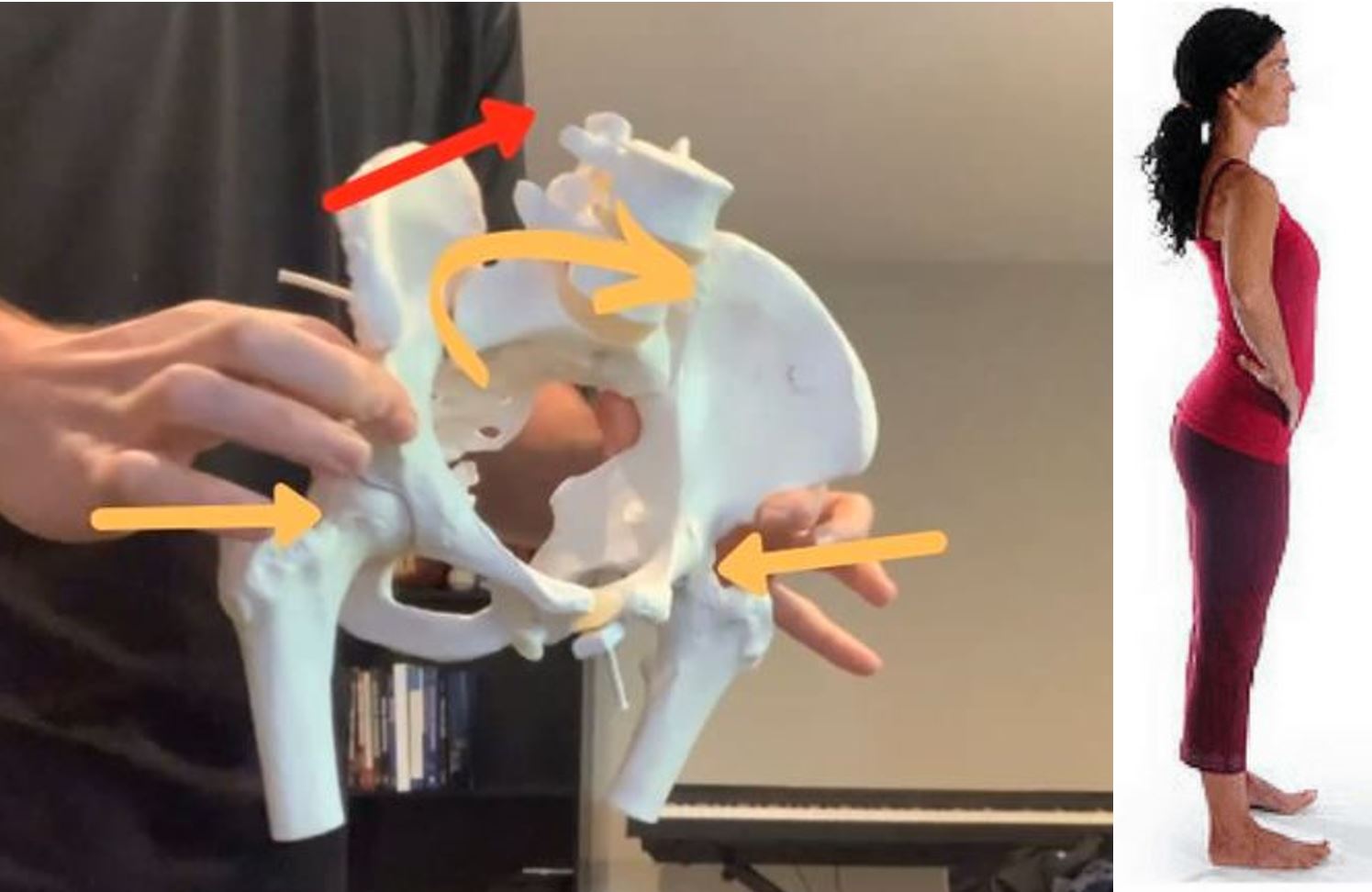
As a result, their ribcage is biased towards a state of internal rotation, and their pelvis toward a state of sacral nutation with the pelvic innominates in extension, adduction, and internal rotation. These individuals also tend to be biased towards foot pronation.
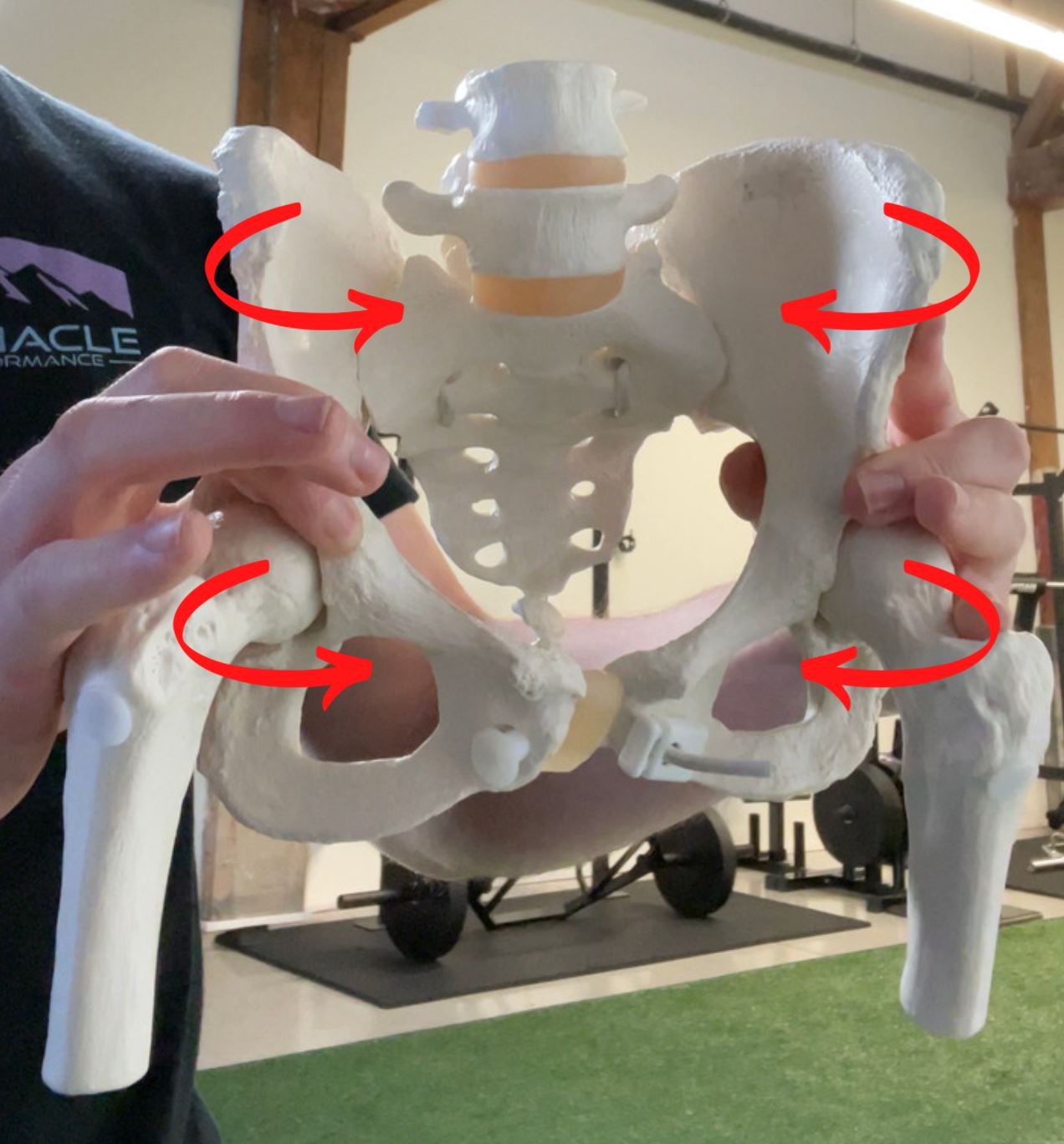
Please note that I am exaggerating the movement of the SI joint and pelvis as a whole for visual illustration purposes. In reality it does not move to this extent, but I am showing more than usual so you can clearly see the movements.
When we exhale, this is a visual of what happens. Wide ISAs are biased here:
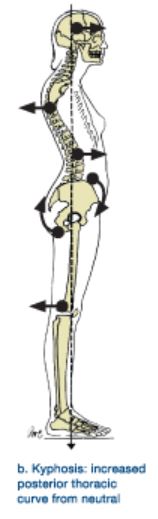
The wide ISA individual typically has exaggerated spinal curves due to the excessive lumbar arch (extension). This is your typical lower/upper crossed syndrome individual.
Narrow Infrasternal Angle Archetype
A Narrow Infrasternal Angle (usually under ~100 degrees but sometimes much less) is a representation of the inverse scenario of the Wide ISA.
These Narrow ISA individuals an individual who has a bias towards inhalation (ribcage ER), and therefore an overly-inflated ribcage.
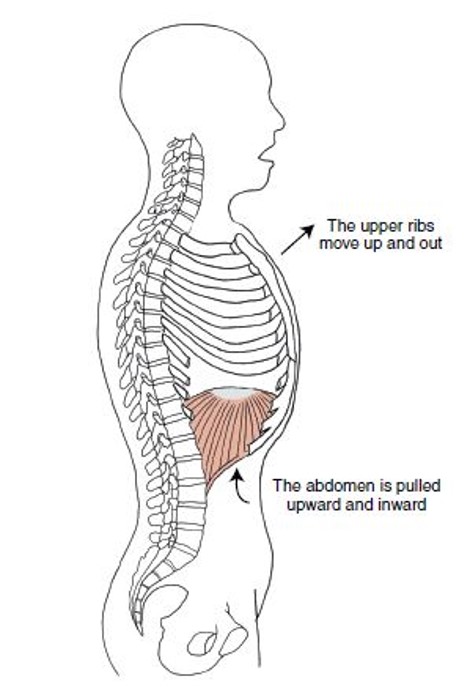
But here’s the thing: their diaphragm is very descended because they are biased towards so much inhalation. When the diaphragm is extremely flattened/descended, two things happen:
- The pressure gradient changes in the ribcage/abdomen
- The line of pull of the muscle on the ribcage changes
Now, when they inhale, the diaphragm still tries to contract and it sucks the abdomen inward and upward (De Troyer):
Their so inhaled that they need to find an exhalation strategy, so they will “close off” their ISA in order to try to push air out. Because of this, you can think of Narrow ISAs being squeezed laterally (side-to-side), while Wide ISAs are being squeezed more front-to-back.
Due to the external rotation bias of their skeleton, they are also biased as a whole (initially) towards the joint actions of:
- Abduction
- Flexion
- Supination
- Plantar Flexion
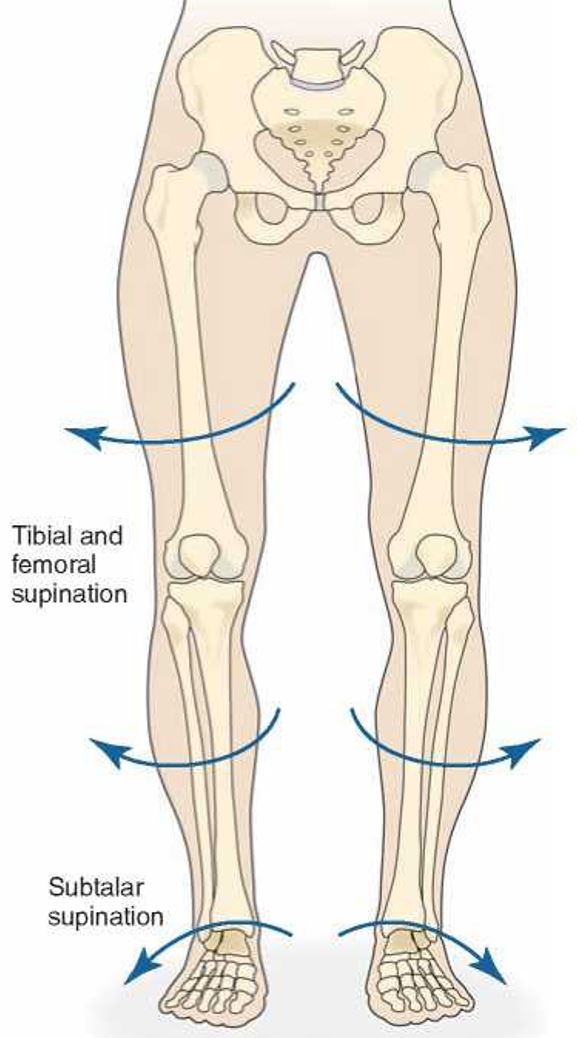
Their pelvis is going to represent what happens when we inhale, which will be counternutation of the sacrum along with external rotation, abduction, and flexion of the innominate bones. Their feet are also going to be more supinated.

When we inhale, this is a visual of what happens. Narrow ISAs are biased here:
Their skeleton will have less spine curves and they will have more of a “flat back” visual presentation. A perfect example of this is a young, more “thin” female with that flat back appearance.

A commonality of both of these ISA archetypes is that the ISA itself is representative of the compensation they have, not their actual bias:
- Wide ISAs have exhaled axial skeletons and therefore seek an inhalation strategy at the ISA via widening it out
- Narrow ISAs have an inhaled axial skeleton and therefore seek an exhalation strategy at the ISA via narrowing it
Asymmetrical Infrasternal Angles
Everyone has a bias towards either a more wide or narrow infrasternal angle, but due to the natural asymmetries of the body, we would expect there to be a degree of asymmetry present in every infrasternal angle. This is additional layer that goes along with this concept, but I will reserve that information for the article I already have on this asymmetrical pattern here.
The short story is, most people will have a slightly more wide left side of their ISA and a relatively more narrow right side.

Common Compensations of Infrasternal Angle Archetypes
Let me preface this by saying that if you recognize yourself in one of these presentations, this is completely normal. Nothing is wrong with you, and everyone has a bias towards one of these presentations due to genetic influences. Imagine a spectrum from a big soman man to a small, marathon running female. Those are the two ends of the spectrum and most people live somewhere in the middle.
The compensations aren’t conceptually that challenging on the surface because it is quite simple: Both of these will try to find their missing joint actions via the path of least resistance.
Common Wide ISA Compensations
We know Wide ISAs are biased towards internal rotation, but in order for humans to move, we have to have external rotation and there really isn’t any way around it.
In order for them to find external rotation and those associated joint actions, they will often create “compression” or tighten things up, on the front side of their body. They’re not going to be able to tighten up what already is tight or shortened, so they’ll have to find it through what is available to them. This results in them pushing their front ribcage down into internal rotation, which results in them depressing their sternum. This will further increase the spine curve of the upper back.

As for their pelvis, they will create compression with muscles on the front side like the adductors to help pull their pelvis forward. Their femurs orient outward and this helps them find external rotation.
Now they will actually present with more external rotation in some areas of their body than internal rotation, which can be confusing to some people, but just understand that this is a compensation to find what they don’t have.
We address this more in detail in the Biomechanics Program, as well as a much deeper dive on what this looks like in terms of specific assessment results.
Narrow ISA Common Compensations
As for the Narrow ISAs, because of their bias towards external rotation, they will try to find internal rotation. The easiest way for them to do this is to create compression in their back to push their pelvis forward in space, which orients their femurs into internal rotation.

This creates that classic “anterior pelvic tilt” appearance:
Because of this, they can present with more internal rotation than external rotation in some measurements, but again, it is a compensation.
The general idea is that both of these types of ISAs will end up going into anterior pelvic tilt, but the way they get there is a little bit different because of their initial bias.
Exercises for Wide ISAs
If you are a Wide ISA, it’s important to know if you have either primary or secondary compensations. I discuss in my Biomechanics Program what these assessments results look like specifically, but generally speaking they will present with limited internal rotation measurements and more external rotation than we would initially expect.
Exercises for Secondary Compensations
Secondary compensations involve bigger muscles closer to the surface of our body. The initial ISA bias is deep within us, meaning muscles like the diaphragm, but also other smaller muscles make up their ability to get into internal rotation more easily. Larger muscles like the adductors, lats, low back extensors, etc, are closer to the surface of our skin and can more easily be recruited as compensatory muscles.
The goal for improving movement in either Wide or Narrows is to first remove the additional layer of compensation. Imagine slicing through the layers of a cake. In order to get to the bottom layer, we need to go through the top one first.
Therefore, we want to take them out of their anterior pelvic tilt first via exercises like the following:
At that point we should have better access to internal rotation and they are more of what we would initially expect for a Wide ISA.
If you're looking for more strategies to improve movement to help your clients feel great, check out my free webinar: 5 Strategies To Help Your Clients Feel 85% Better Immediately
Exercises for Primary Compensations
If we are working with a primary compensation layer, we want to restore external rotation and promote use of the obliques to help close off the ISA and improve posterior ribcage expansion.
We want do that via exercises such as:
As for loaded exercises, they will benefit from more squat-like positions that help promote external rotation such as:
Exercises for Narrow ISAs
Narrow ISAs need a similar strategy – take them out of secondary compensations first (anterior pelvic tilt), and then restore external rotation based measurements.
A lot of the same types of drills will work to help “bring their pelvis back”, but because Narrow ISAs will posteriorly compress, it is often helpful to inhibit and reduce tone in the muscles that get tight in the mid/upper back:
Exercises for Primary Compensations
Narrow ISAs without additional compensations will need more internal rotation and anterior ribcage expansion, so we can help improve that with exercises such as:
As for loaded exercises, they will benefit from more hinge-like positions that help promote internal rotation such as:
Third Layer of Compensations
The interesting thing about these layers of compensation is that the deeper either ISA goes, the more they tend to look the same. A good example this is imagining a 90-year old person on a walker. They tend to have this "swayback" posture because they've had decades of time to live under the influence of gravity while eventually slowly losing the ability to remain upright against it via losses of muscle mass, coordination, mobility, etc.
I have a full article and video on this concept here.
Summary
Hopefully this is a very helpful framework for you to understand certain genetic biases and layers of compensation can be added on top of them over time.
There are additional layers and more intricacies, which I cover in my Biomechanics Program, but this article is a great starting point if you are new to this idea.
The general concept is we all start biased more or less towards one end of the spectrum of Wide or Narrow ISA, and over time we will seek to find what we don’t have via the path of least resistance. The result of the compensations is often an ability to access some degree of what was missing, but at the cost of limitations in the original bias.
Peel back the layers of compensation one at a time, then you can fill in the gaps after that.
Don’t miss out on free education
Join our email list to receive exclusive content on how to feel & move better.
